Specific Abnormalities

Abnormal scan results? We make sure you are fully informed
Nobody wants to be told they have a heart condition; we believe a more complete understanding empowers you to take the next steps.
Understanding your results in detail.
Echo scans are reported according to internationally established guidelines. As a consequence, the scan results contain numerous technical terms, figures and calculations, which can be readily interpreted by Heart Specialists all over the world, but can be confusing for the non-expert. An explanation of the key anatomical terms and scan findings follows below.


If you need further information on specific cardiac abnormalities, you can find it here.
Search for answers here:
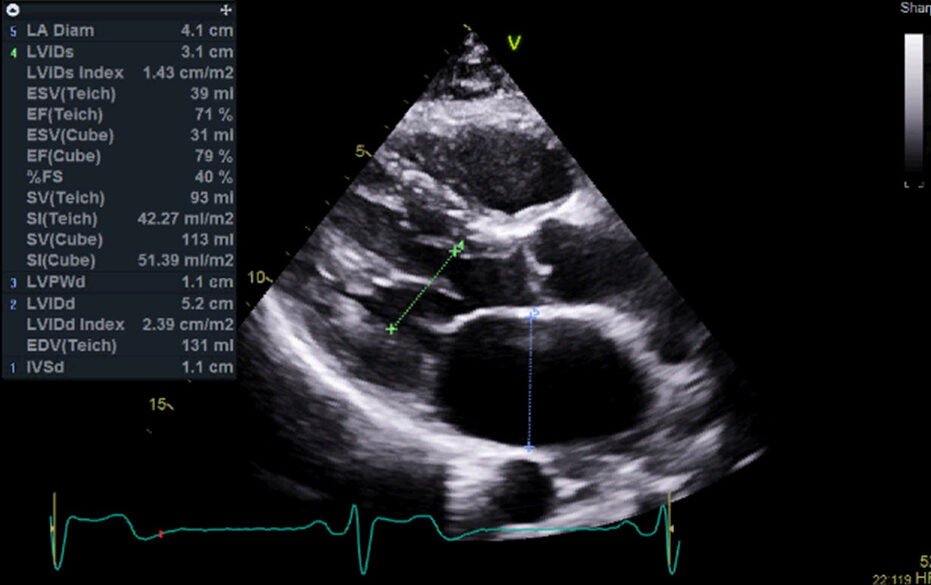
Chamber size abnormalities occur when your heart's four chambers become enlarged or smaller than normal, affecting blood flow efficiency. This commonly happens due to high blood pressure forcing the heart to work harder, valve problems, or heart muscle disease.
You might experience shortness of breath, fatigue, or palpitations, though mild cases often show no symptoms.
Complete Guide About Chamber Size Abnormalities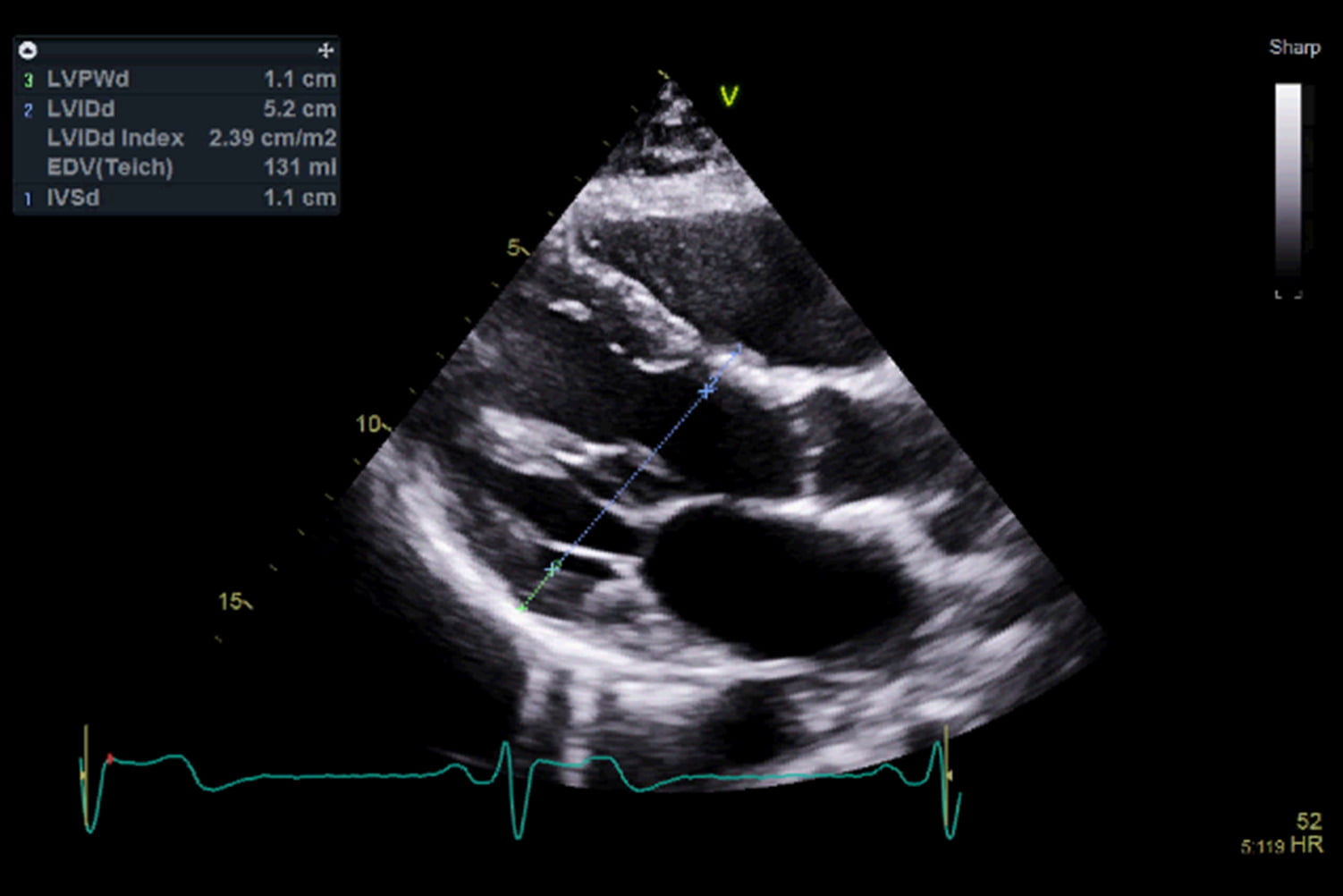
Ventricular wall thickness abnormalities occur when the muscular walls of your heart's main pumping chambers become abnormally thick or thin. The most common issue is left ventricular hypertrophy, where the wall thickens due to high blood pressure or valve problems, forcing the heart to work harder. This can also happen from genetic conditions like hypertrophic cardiomyopathy, or conversely, walls can become too thin in dilated cardiomyopathy.
Symptoms include shortness of breath during activity, chest pain, palpitations, and fatigue. Your echocardiogram measures wall thickness precisely, with normal left ventricular walls ranging from 6 to 11 millimetres.
Complete Guide About Ventricular Wall Thickness Abnormalities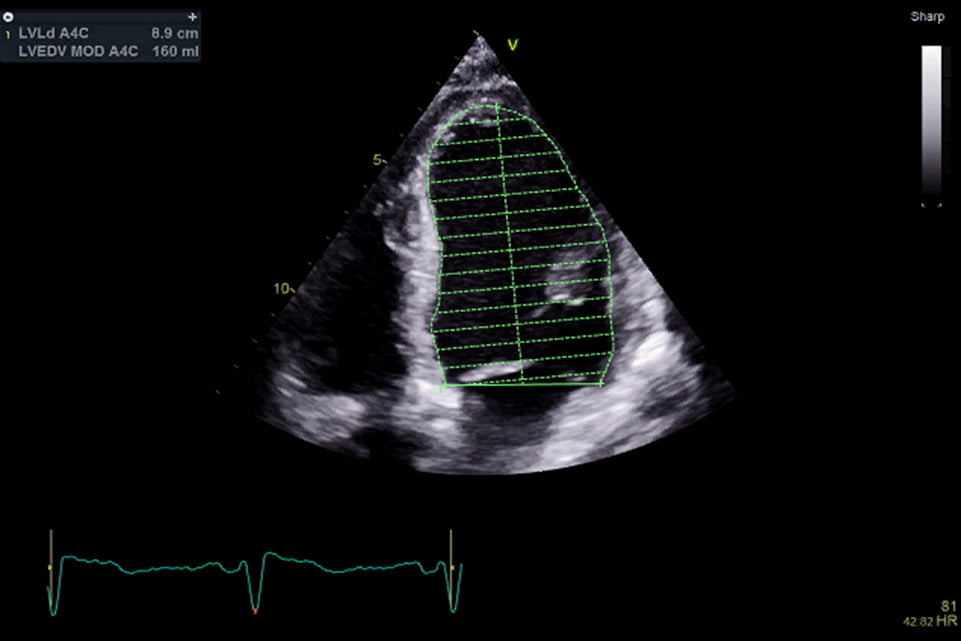
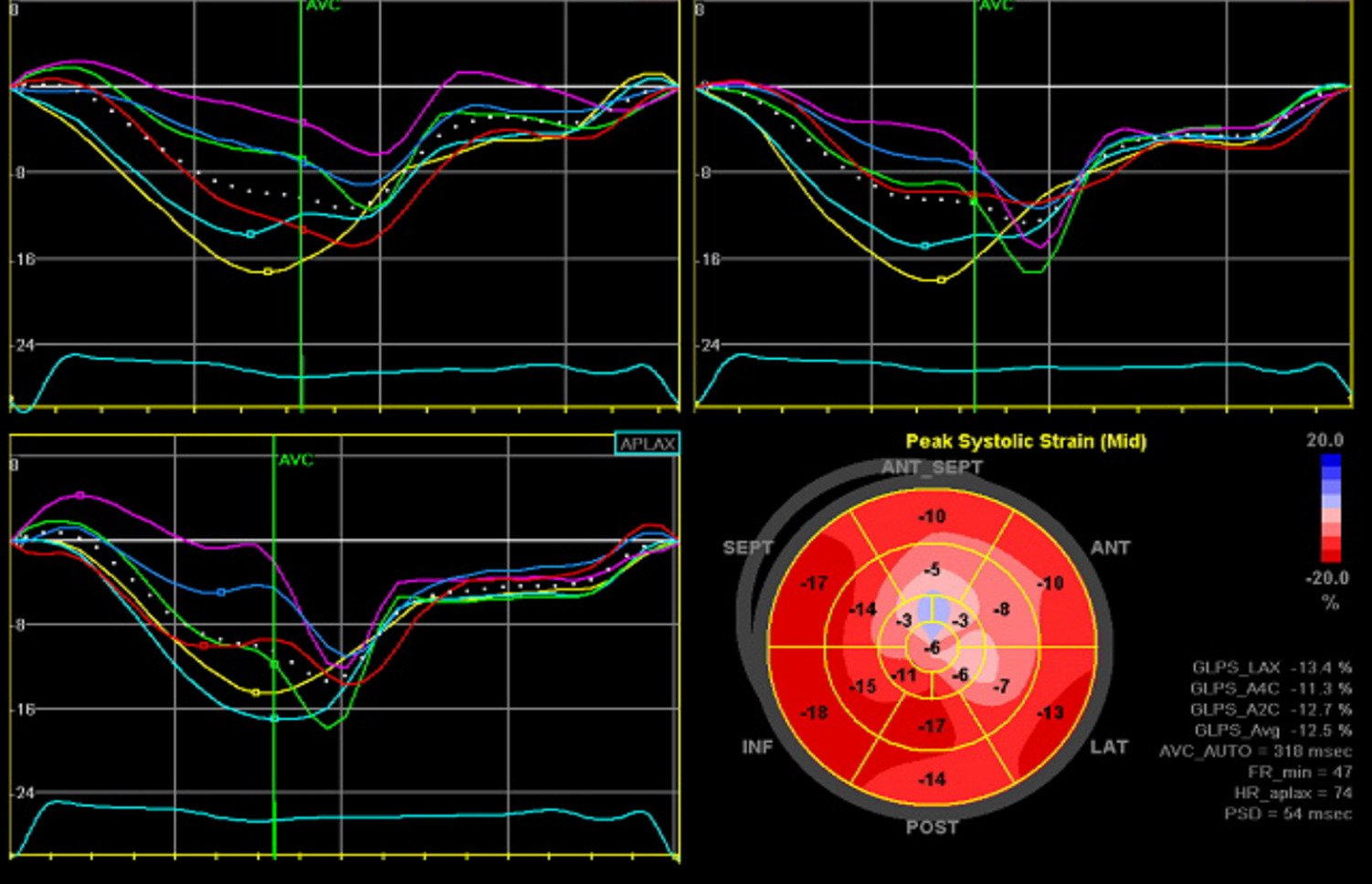
Systolic function abnormalities occur when your heart's pumping ability becomes impaired, reducing the amount of blood ejected with each heartbeat. This is measured by ejection fraction, with normal hearts pumping out 50-70% of blood from the left ventricle. Impaired systolic function is classified as mild (40-49%), moderate (30-39%), or severe (below 30%).
Common causes include heart attacks, coronary artery disease, high blood pressure, and heart muscle diseases. You may experience shortness of breath during activity, persistent fatigue, leg swelling, and exercise intolerance.
Complete Guide About Systolic Function Abnormalities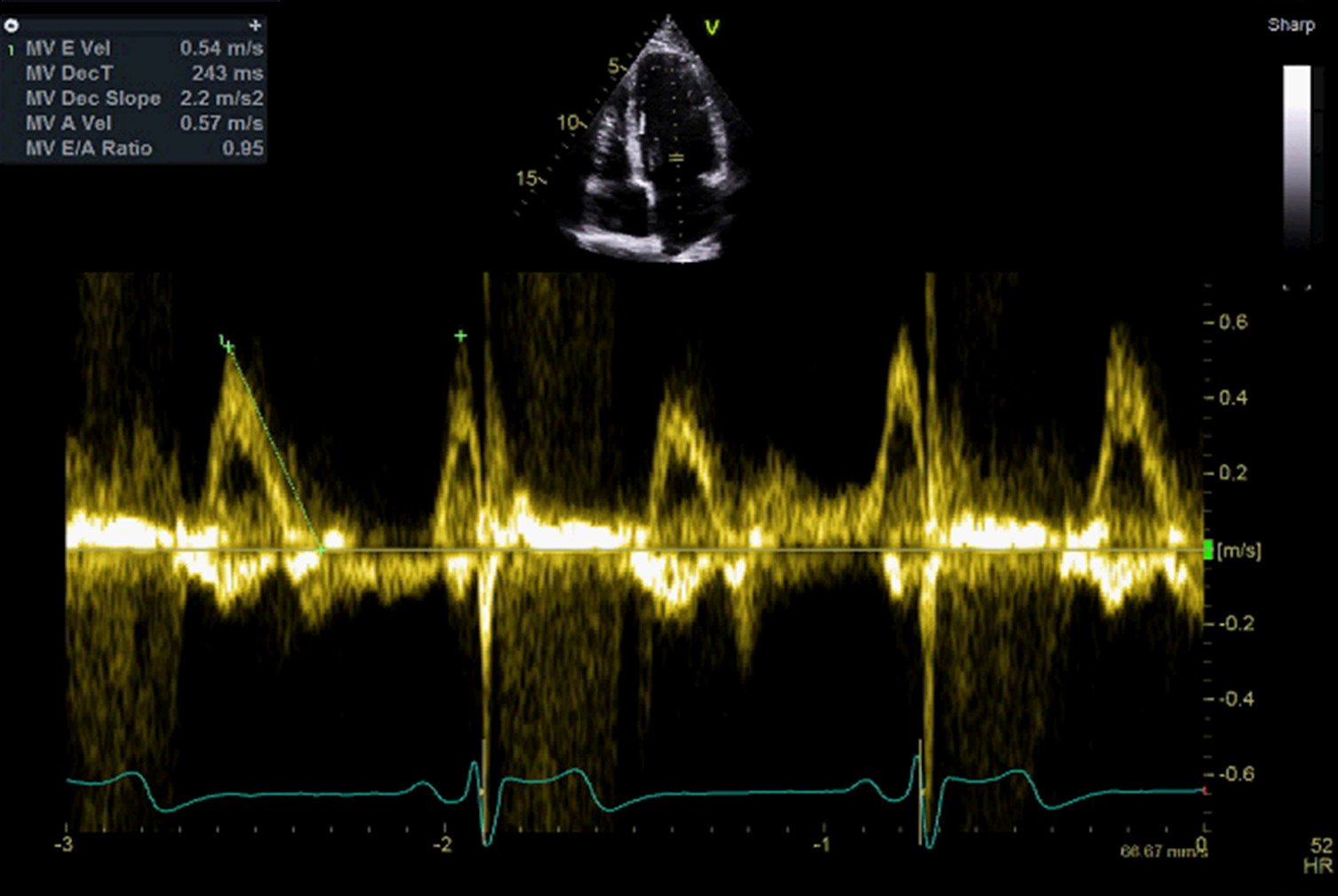
Diastolic function abnormalities occur when your heart's ventricles struggle to relax and fill with blood between heartbeats. This is classified into three grades: mild (impaired relaxation, often no symptoms), moderate (pseudonormal filling with shortness of breath and fatigue), and severe (restrictive filling with heart failure symptoms). Unlike systolic problems, where the heart can't pump effectively, diastolic dysfunction means your heart pumps normally but can't fill correctly.
Common causes include high blood pressure leading to stiff heart walls, ageing, diabetes, and coronary artery disease. Symptoms include shortness of breath during activity or lying down, persistent fatigue, and leg swelling.
Complete Guide About Diastolic Function Abnormalities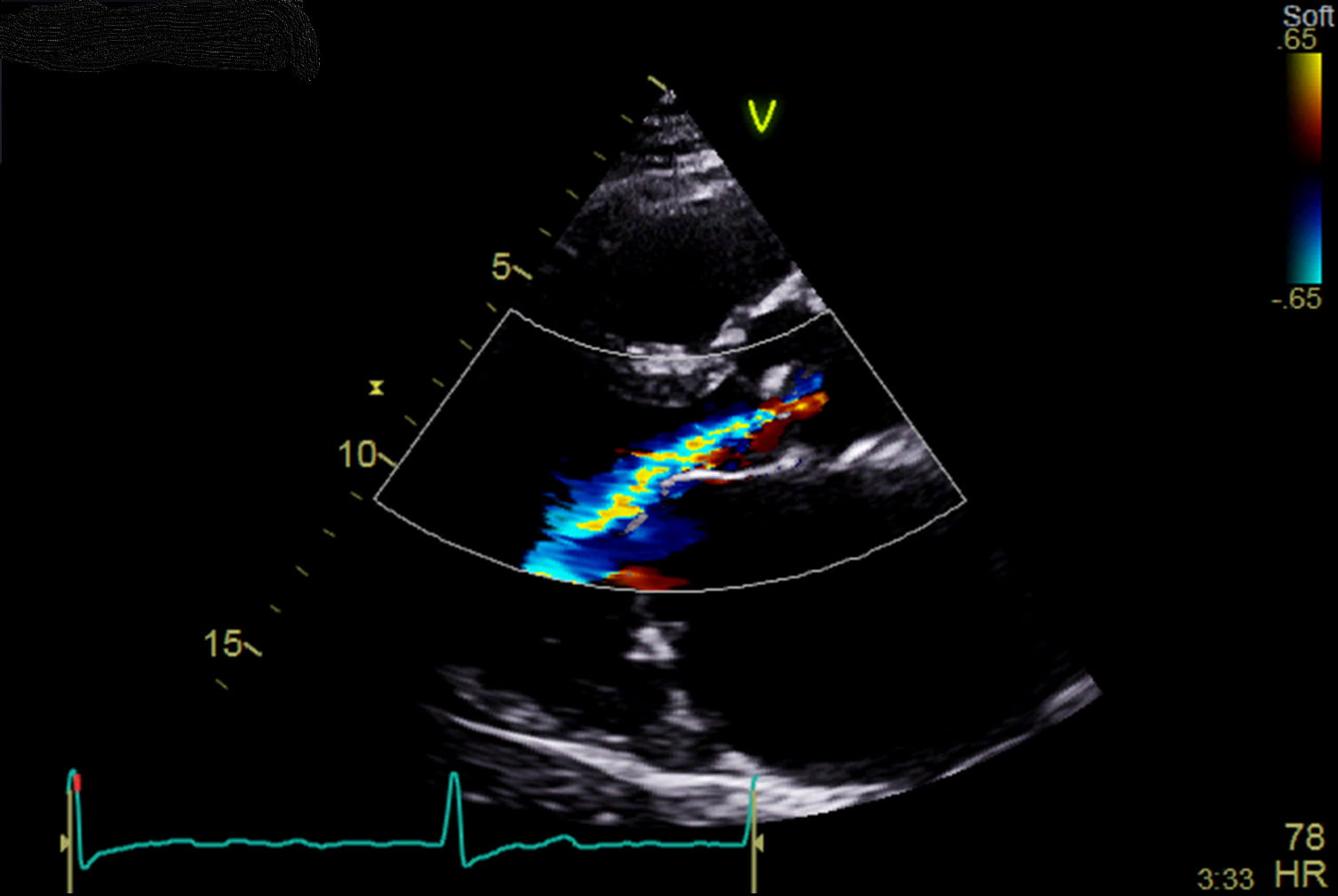
Valve regurgitation occurs when one or more of your heart's four valves fail to close properly, allowing blood to leak backwards instead of flowing forward efficiently. The most common types are mitral regurgitation (between the left chambers) and aortic regurgitation (from the main artery back into the left ventricle), though tricuspid and pulmonary valve leakage can also occur.
Mild cases often cause no symptoms, but moderate to severe regurgitation can lead to shortness of breath, fatigue, heart palpitations, leg swelling, and chest pain. Common causes include age-related wear, congenital defects, infections like endocarditis, rheumatic fever, and high blood pressure damage. Your echocardiogram visualises valve movement and uses colour Doppler to measure the degree of backwards blood flow, grading severity from mild to severe.
Complete Guide About Value Regurgitation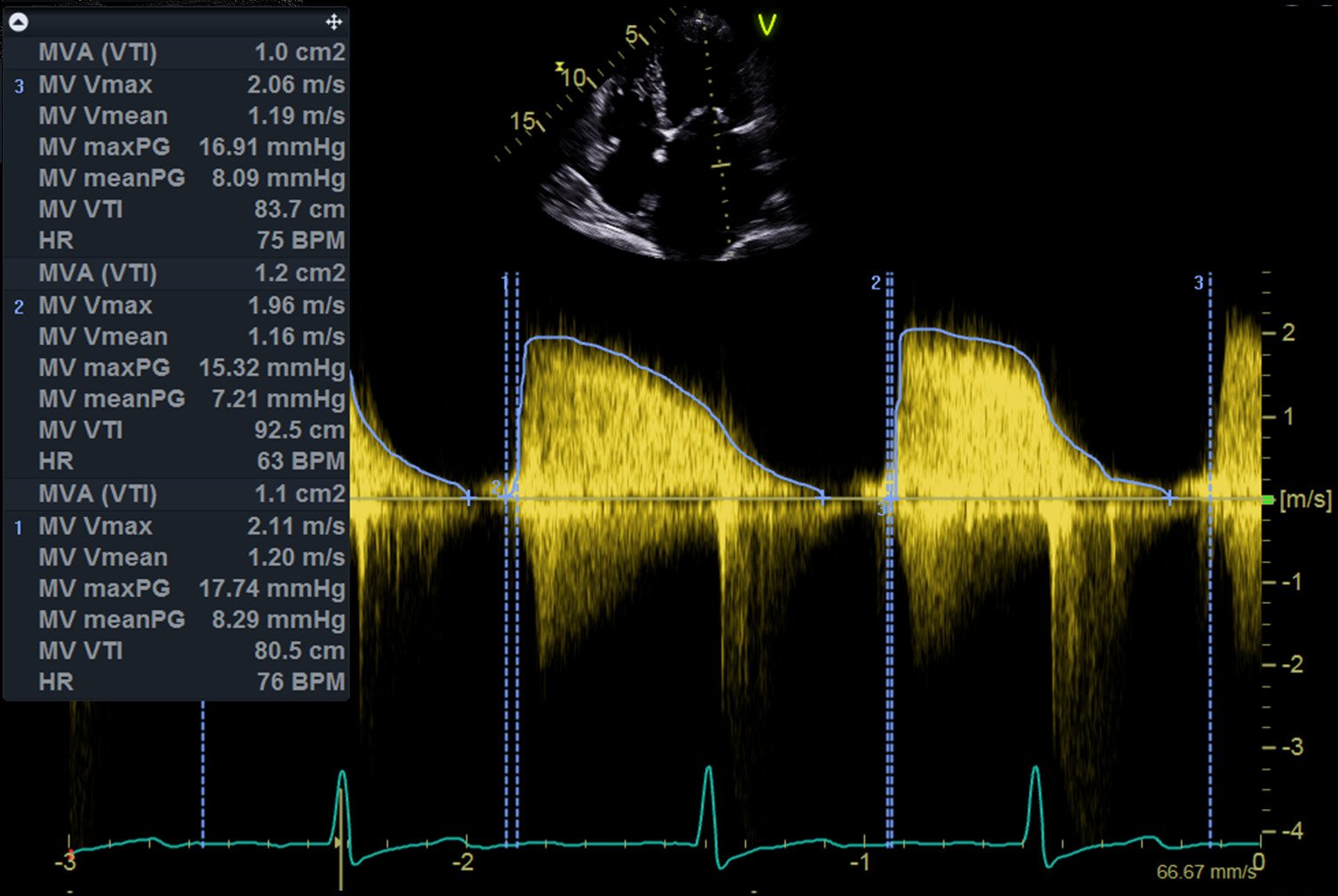
Valve stenosis occurs when one of your heart's four valves becomes narrowed, restricting blood flow and forcing your heart to work harder. The most common types are aortic stenosis (narrowed main outlet valve) and mitral stenosis (narrowed valve between the left chambers), classified as mild, moderate, or severe based on the degree of narrowing.
Symptoms include shortness of breath during activity, chest pain, fatigue, heart palpitations, and dizziness or fainting with exertion. Common causes include age-related calcium deposits on valves, congenital defects, rheumatic fever damage, and radiation therapy effects. Your echocardiogram measures how well valves open and close, with additional CT scans showing calcium buildup and cardiac catheterisation measuring pressure differences across narrowed valves to determine severity.
Complete Guide About Valve Stenosis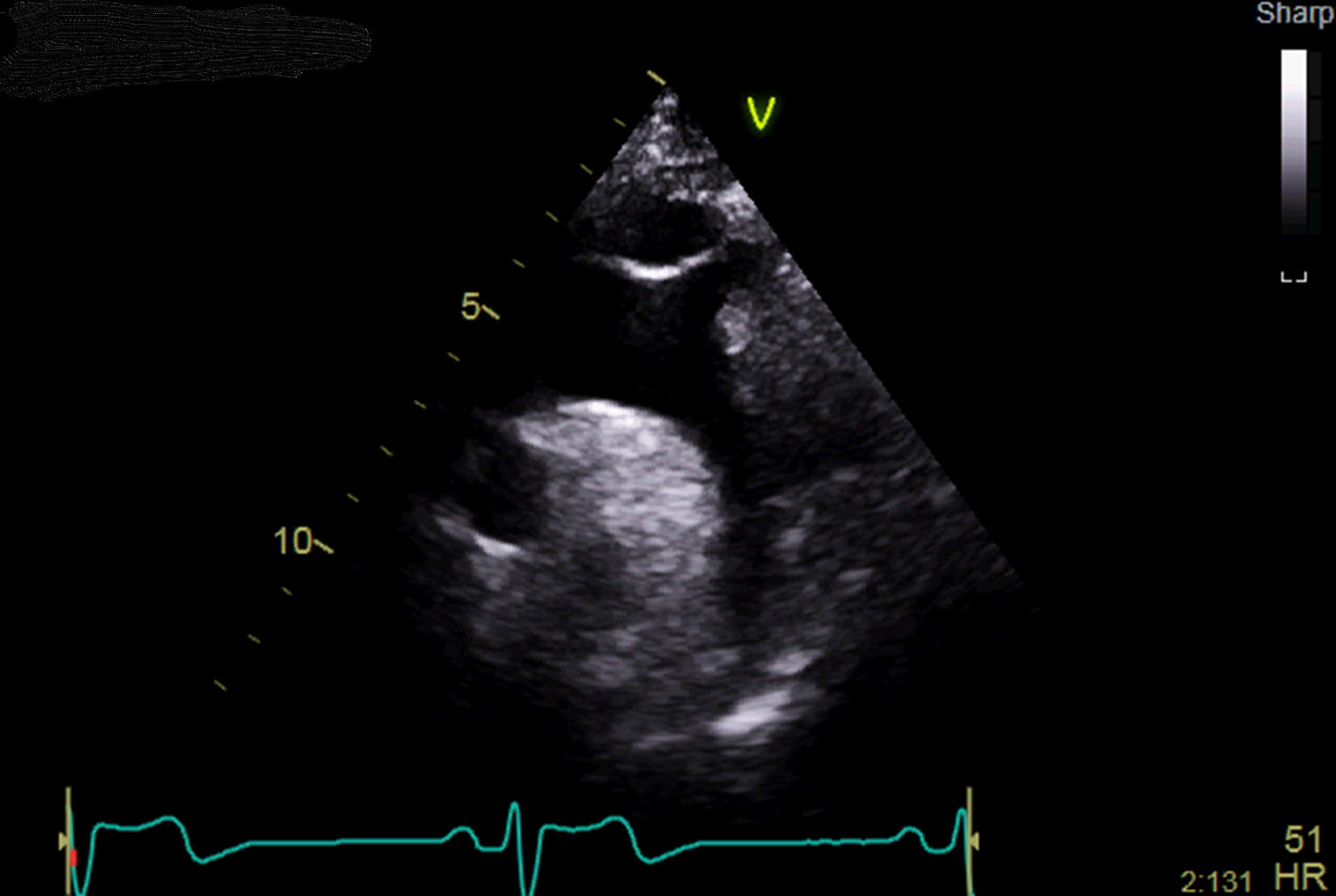
Aortic abnormalities affect the main artery that carries blood from the left ventricle to the rest of the body. The most recognised conditions include aortic dilation or aneurysm (progressive enlargement), aortic dissection (a tear in the vessel wall), and coarctation (a congenital narrowing). These can develop silently or be linked to high blood pressure, connective tissue disorders, or valve disease, such as a bicuspid aortic valve.
Symptoms may include sudden chest, back, or abdominal pain, shortness of breath, dizziness or fainting, and, in abdominal aneurysms, a pulsating feeling in the tummy. Many cases, however, are found only on imaging. An echocardiogram can evaluate the aortic root and the start of the ascending aorta, while CT or MRI provide detailed views of the whole vessel and helps plan treatment.
Complete Guide About The Aorta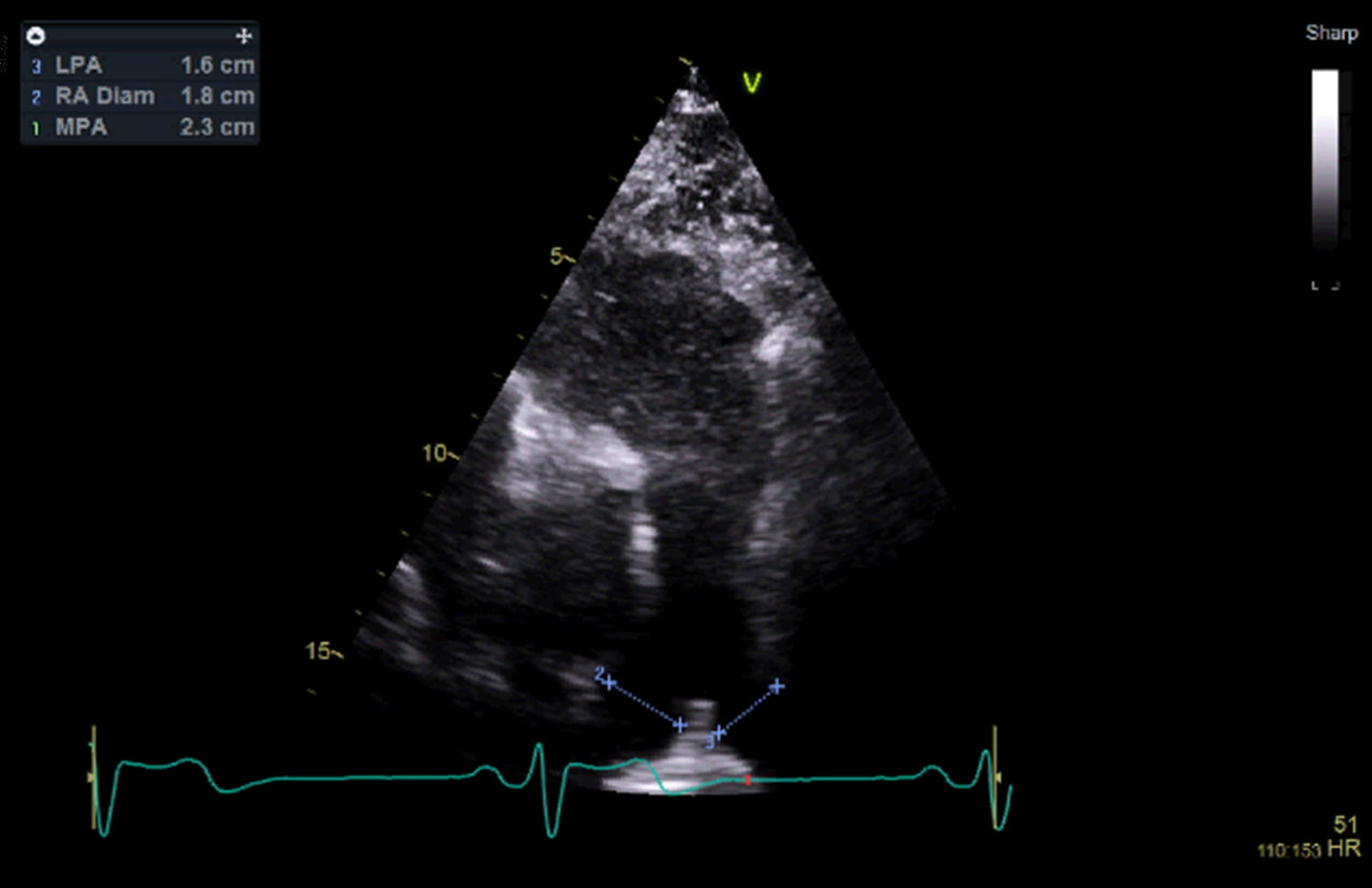
Pulmonary artery abnormalities affect the blood vessels that carry blood from your heart's right ventricle to your lungs for oxygenation. The most serious conditions include pulmonary arterial hypertension (high blood pressure in lung arteries), pulmonary embolism (blood clots blocking these arteries), and pulmonary artery enlargement from chronic pressure or lung disease.
Symptoms include shortness of breath during activity, fatigue from reduced oxygen delivery, chest pain, heart palpitations, and swelling in the ankles or abdomen, indicating right heart strain. These conditions can be severe and life-threatening if left untreated. Your echocardiogram assesses pulmonary artery size and right heart function, while CT pulmonary angiography provides detailed images to detect blockages and measure arterial dimensions.
Complete Guide About The Pulmonary Arteries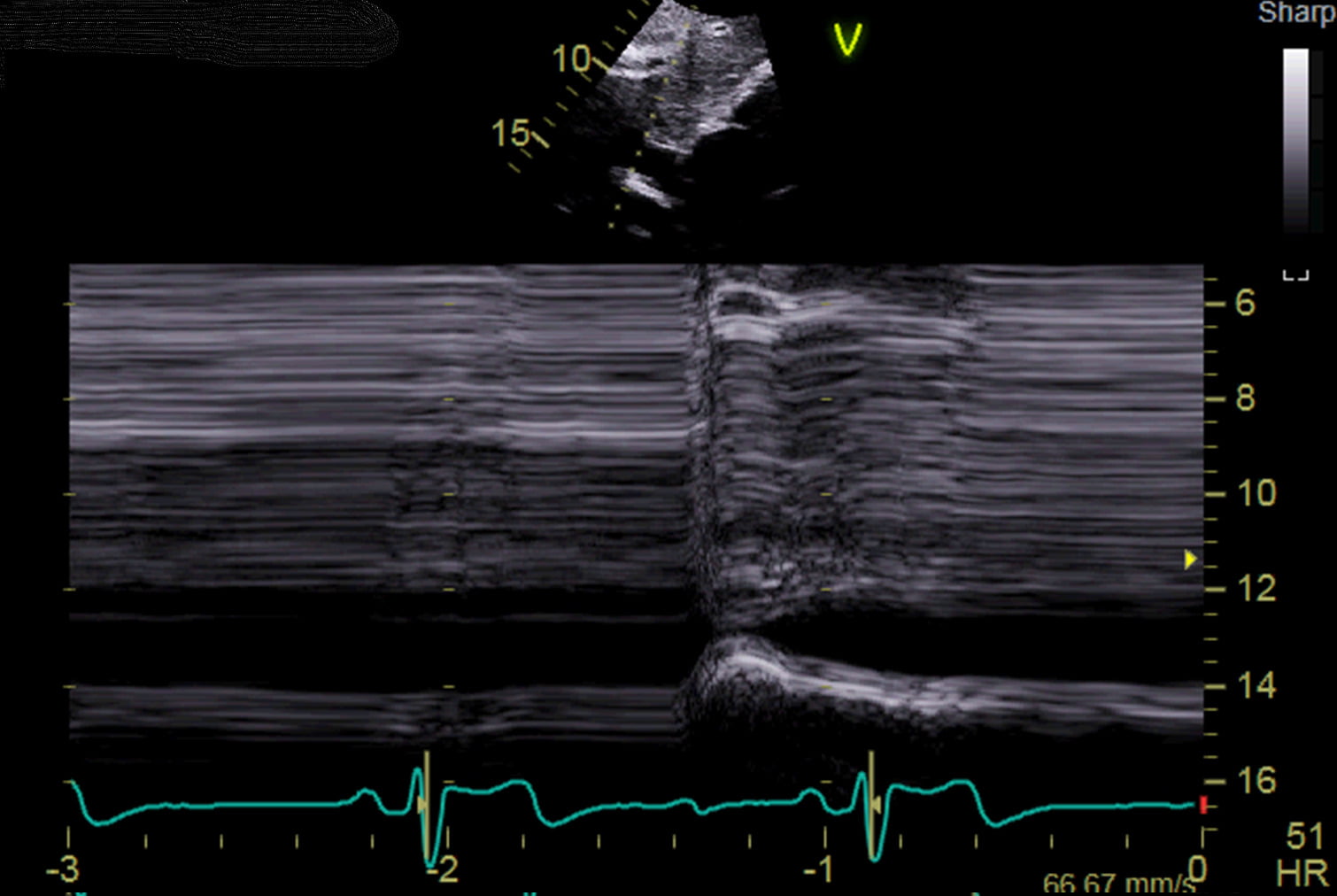
Inferior vena cava abnormalities affect the large vein that returns blood from your lower body back to your heart. Common problems include obstruction from blood clots or tumours, thrombosis (clot formation within the vein), and collapse from external compression or dehydration.
Symptoms include swelling in the legs and lower body due to impaired blood return, leg or back pain, shortness of breath if clots travel to the lungs, and fatigue from compromised circulation. Causes range from blood clots due to prolonged immobility, tumours compressing the vein, congenital abnormalities, and trauma to the abdomen or pelvis. Your echocardiogram can visualise the inferior vena cava as it enters your heart, while ultrasound, CT, and MRI provide detailed images to detect blockages or structural problems.
Complete Guide About The Inferior Vena Cava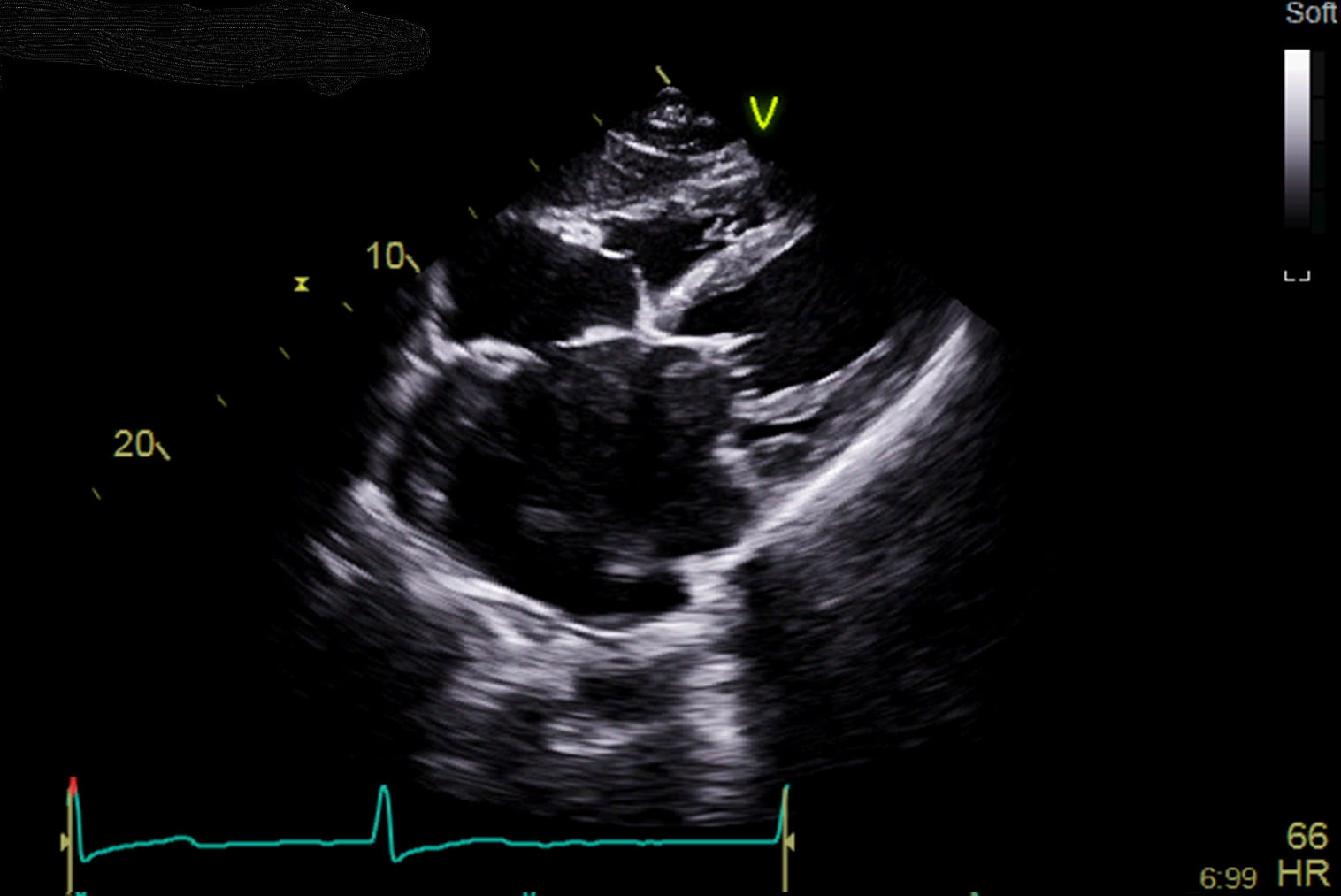
Pericardial abnormalities affect the double-layered protective sac surrounding your heart. Common conditions include pericarditis (inflammation causing sharp chest pain), pericardial effusion (excess fluid buildup), constrictive pericarditis (scarring that restricts heart movement), and cardiac tamponade (severe fluid compression requiring emergency treatment).
Symptoms include sharp chest pain that worsens with breathing or lying down, shortness of breath, heart palpitations, fatigue, and sometimes fever with inflammatory conditions. Causes range from viral or bacterial infections, autoimmune disorders like lupus, heart attacks, chest trauma, cancer, and complications from heart surgery or radiation therapy. Your echocardiogram is the primary tool for detecting fluid around the heart and assessing pericardial function, while an ECG can identify characteristic changes associated with pericarditis.
Complete Guide About The Pericardium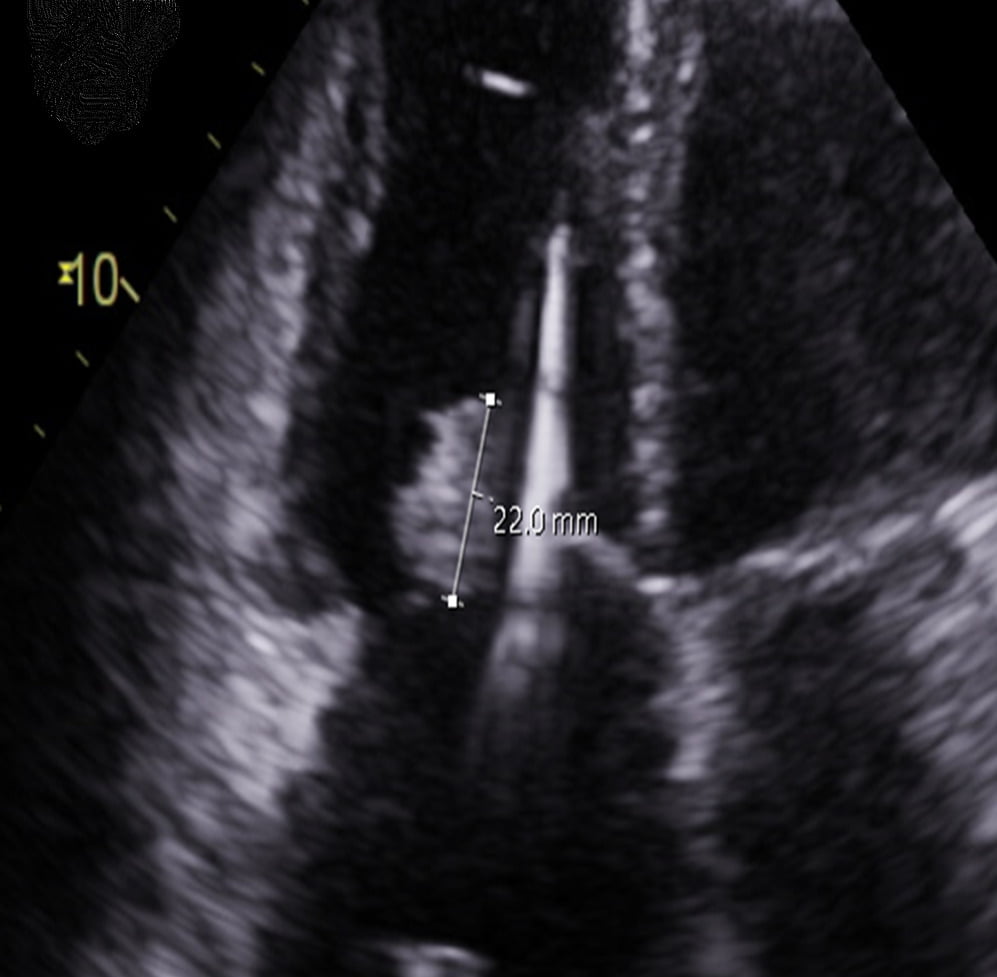
Masses attached to heart valves are abnormal growths or formations that develop on valve structures, including benign tumours like papillary fibroelastomas, malignant tumours such as sarcomas, vegetations from infective endocarditis, and blood clots (thrombi). These can cause serious complications, including valve obstruction, stroke from emboli breaking off and travelling to the brain, and sepsis from infections. Symptoms include chest pain, shortness of breath, heart palpitations, fever, malaise with infections, and fatigue from reduced heart function.
Common causes include bacterial or fungal heart infections, genetic predisposition for certain tumours, underlying heart conditions like atrial fibrillation promoting clot formation, and primary or metastatic cancers. Your echocardiogram, particularly transesophageal echo (TEE), provides detailed images of valve structures to identify these masses, while cardiac MRI and CT scans help distinguish between different types.
Complete Guide To Heart Valve Masses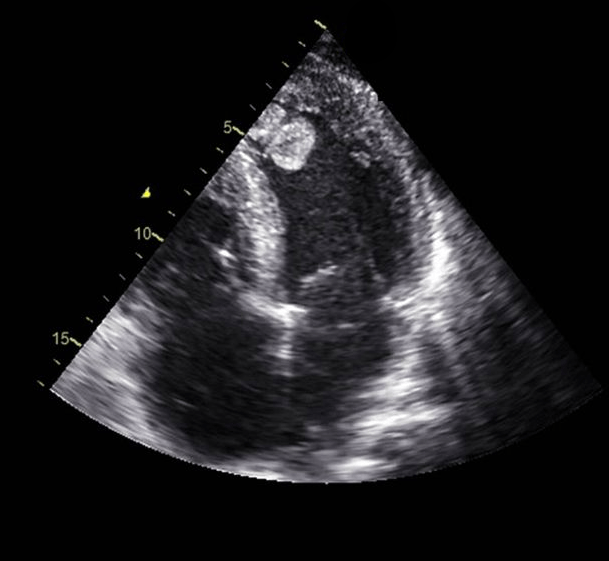
Primary cardiac tumours (such as a left atrial myxoma) are extremely rare. If your scan is suspicious for a tumour, you will be referred for specialist investigation.
A blood clot (or thrombus) is an unusual finding in the heart, but can be encountered in patients with a recent heart attack or in cases of very severely reduced systolic function. These cases will need a referral for blood-thinning medication consideration. Very small blood clots can be difficult to see on a standard cardiac ultrasound; if there is any doubt, you may be referred for consideration of an alternative imaging test.
Complete Guide About Mass Elsewhere in the Heart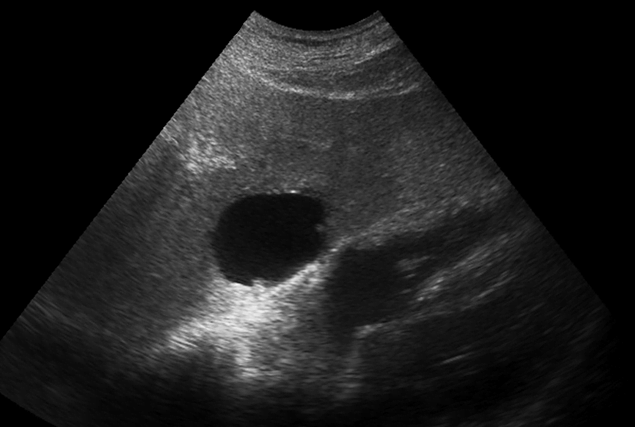
Extracardiac abnormalities affect blood vessels, structures, and tissues surrounding your heart that can significantly impact cardiovascular health. Common conditions include aortic aneurysms (abnormal bulging of the main artery that can be life-threatening if ruptured), pulmonary embolism (blood clots blocking lung arteries), pericardial effusion (excess fluid around the heart), and coarctation of the aorta (congenital narrowing). Your scan may also detect incidental findings like liver lesions, which are usually benign cysts.
Symptoms include chest pain, shortness of breath, limb swelling, dizziness, and coughing. Causes range from genetic factors and lifestyle choices like smoking to infections, trauma, blood clotting disorders, and inflammatory diseases. Your echocardiogram can visualise surrounding structures, while CT and MRI scans provide detailed images of blood vessels and tissues outside the heart.
Complete Guide About Abnormalities of the Heart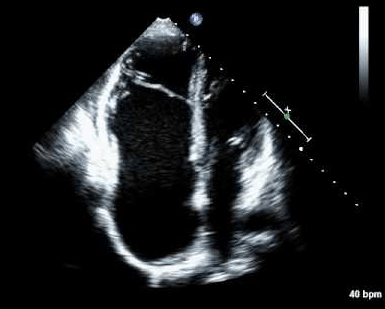
Congenital heart disease refers to structural heart abnormalities present from birth, affecting the heart's walls, valves, or blood vessels. While significant abnormalities are usually identified in childhood, your scan may detect previously undiagnosed defects such as holes in the heart (septal defects). These range from critical conditions requiring immediate intervention, like hypoplastic left heart syndrome, to non-critical defects like atrial or ventricular septal defects that may cause symptoms later in life. Common signs include bluish skin (cyanosis), shortness of breath, heart murmurs, poor feeding and growth in infants, fatigue, and swelling.
Causes involve genetic factors, chromosomal abnormalities like Down syndrome, and environmental influences during pregnancy such as maternal diabetes, infections, or medication exposure. Your echocardiogram can identify structural abnormalities, while foetal echocardiography during pregnancy allows early detection and planning for immediate postnatal care.
Complete Guide About Congenital Heart DiseaseNon-valvular cardiac masses include tumours and blood clots that form within heart chambers or on heart walls. The most common are atrial myxomas, benign tumours typically arising from the left atrium that, despite being non-cancerous, can cause serious complications through blood flow obstruction and embolism. Thrombi (blood clots) are particularly dangerous as they can break off and cause strokes, heart attacks, or pulmonary embolism, often forming in the left ventricle after heart attacks or in atria during irregular heart rhythms like atrial fibrillation.
Symptoms include chest pain, shortness of breath, heart palpitations, and embolic events such as sudden weakness or speech difficulties from stroke. Atrial myxomas require surgical removal (myomectomy), while thrombi are treated with anticoagulant medications to prevent further clotting and help dissolve existing clots. Your echocardiogram can detect these masses, with transesophageal echocardiography (TEE) providing more detailed internal imaging.
Complete Guide About Cardiac MassesBook Your Heart Scan Today